Introduction
Physiotherapy in Hamilton West Mountain & Ancaster for Shoulder
Welcome to Westmount Physiotherapy’s guide to adult humerus fractures.
The humerus goes from the shoulder joint to the elbow joint and must be strong enough to take a good deal of weight when you lift something or push against something. It is one of the big three bones of the body. Only the femur (thighbone) and the tibia (shinbone) are bigger and stronger. Without a functioning humerus you cannot position the hand in space or use the elbow.
It takes quite a lot of force to break the humerus and this is a serious injury that almost completely eliminates the functions of the arm. On the plus side, because it is surrounded by muscle, the bone's blood supply is excellent and it has a good reputation for healing.
This guide will help you understand:
- what parts of the arm are involved
- what the symptoms are
- what can cause these fractures
- how health care professionals diagnose these fractures
- what the treatment options are
- what Westmount Physiotherapy’s approach to rehabilitation is
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Shoulder Pain|limit:15|heading:Hear from some of our patients who we treated for *Shoulder Pain*#
Anatomy
What structures are most commonly injured?
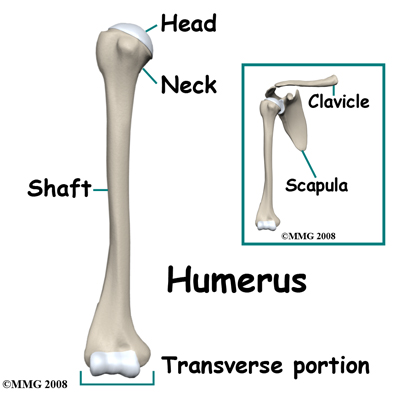 At the shoulder the has a rounded end (the humeral head) that forms part of the shoulder joint.
At the shoulder the has a rounded end (the humeral head) that forms part of the shoulder joint.
It is joined to the shaft of the bone by a region called the neck of the humerus. Most of the shaft of the bone is tubular but it flattens out at the lower end.
The upper arm is so muscular that it is quite difficult to feel the actual bone. In this guide we are concerned with injuries to the tubular shaft of the humerus.
The shaft of the humerus can be broken almost anywhere along its length, although a fracture is more common at the middle of the shaft and below.
There are different patterns of fracture depending on the mechanism of injury, but all involve a complete break around the entire circumference of the tubular bone. In adults it is virtually impossible to break the tube on one side only. This is significant because it means that any break of the humerus interrupts the function of the arm. You cannot lift up or rotate the arm below the break.
Related Document: Westmount Physiotherapy's Guide to Shoulder Anatomy
Shoulder Anatomy Introduction
Causes
How do fractures of the humerus commonly happen?
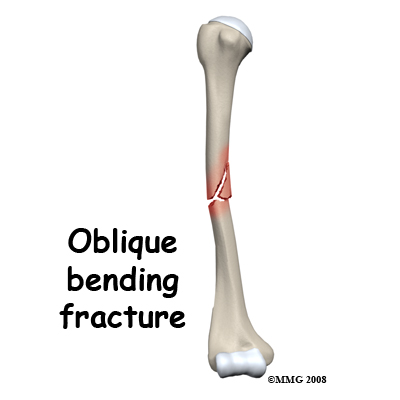
Like any of the big long bones of the body the force that breaks the humerus can be bending, compressing, or twisting. A combination of these forces is the most common. An impact against the upper arm that causes a bending force on the bone is the least common mechanism of injury. This type of injury does occur in high-energy trauma, such as motor vehicle accidents or falls from a height.
Indirect bending forces occur when you fall on the outstretched hand or the elbow. This is a relatively common cause of an isolated humerus fracture and occurs quite frequently in the elderly. In the elderly, the bone may be more fragile than normal due to osteoporosis so can break with falls that would normally seem harmless.
Types
What types of fractures are there?
 Because of the thick layers of muscle around the shaft of the humerus, open fractures are uncommon.
Because of the thick layers of muscle around the shaft of the humerus, open fractures are uncommon.
Open occur with high-energy impact injuries and with gunshot wounds but are much less common with lower energy events such as falls and throwing injuries.
Pathological fractures through abnormal bone occur frequently in osteoporosis and may also happen if there is a deposit of cancer in the shaft of the humerus.
This is a rare event but may be the first sign of the cancer in some people.
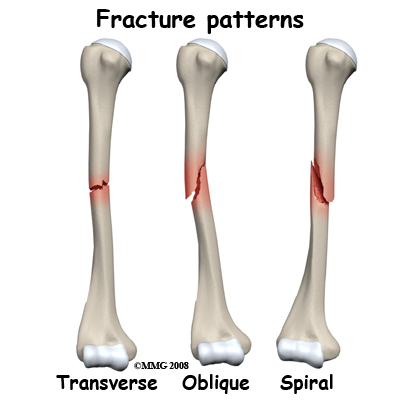
Fractures of the shaft of the humerus that occur from bending forces may have a short oblique pattern or may have multiple fragments.
Compression fractures happen when the force is primarily along the line of the bone.
This can occur in a fall from a height. The fracture pattern is often transverse.
Twisting injuries result in a spiral fracture pattern in the shaft of the humerus. This can happen when the lower arm is locked or trapped in machinery and the body rotates. Direct twisting forces as in arm wrestling have been known to cause spiral fractures as has throwing. Throwing grenades during military training has a particularly high incidence of spiral fracture of the humerus!
The soft tissue injured around a humerus fracture may be considerable. After the bone breaks the sharp ends tear through nearby structures such as muscle and even nerves or blood vessels. The radial nerve that supplies the muscles that straighten the wrist and fingers runs next to the shaft of the humerus. It is quite vulnerable to injury. Other nerves and major blood vessels are more rarely damaged but may be injured as part of a gunshot wound or a major laceration.
Symptoms
What symptoms do humerus fractures cause?
Sudden severe pain following an accident or a sudden force on the upper arm is characteristic of a fracture. The lower part of the arm will go limp because the lower part of the arm is uncontrollable. This may cause a lot of pain at the fracture site when it moves. It is common for the patient to hold the elbow or forearm still, splinting it against the body. The pain is made worse by attempting to move the arm or by passive movements of the lower arm. There may be deformity of the upper arm with an obvious bend in the bone.
If there is an open fracture the wound is usually obvious and the bone ends may be seen. Even a small laceration in the presence of a fracture should raise suspicion of an open fracture. The fracture site will swell rapidly after the accident as the bone and muscle bleeds into the tissues. Purple discoloration and bruising are seen within hours of the injury.
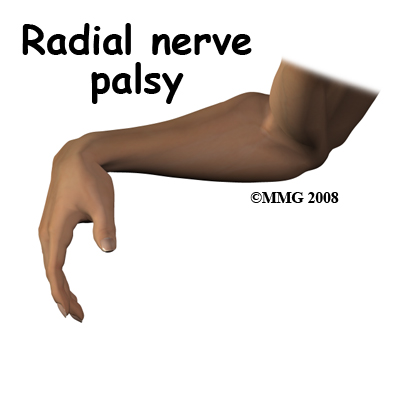
In the more rare situations where there has been an injury to a nerve, the patient will have numbness and loss of movement below the break. The most common pattern is lack of movement of the muscles supplied by the radial nerve. The patient is unable to extend, or lift the wrist and straighten the fingers. This is called a wrist drop. If blood vessels have been damaged the hand may become cold and numb. The pulse at the wrist may not be present.
Even after treatment to stabilize the fracture there will be continuing symptoms of pain, tenderness, swelling, bruising and pain on moving the arm. These are caused in large degree by the injury to the muscles around the broken bone and by the bleeding into the tissues caused by the break. These symptoms will continue for several weeks but do gradually get better. Increasing pain, a change in the quality of the pain, or the new development of numbness would be a cause for concern and should be reported to your Doctor.
Evaluation
How will my fracture be evaluated?
First aid at the scene of the accident would usually consist of treating shock, applying dressings to wounds if needed, and splinting the arm. An ordinary sling will help quite a bit but wrapping a bandage all the way around the chest to bind the arm to the side of the trunk may relieve the pain more completely. The patient should be transferred to the hospital for definitive treatment as soon as possible.
In the Emergency Department the focus will be on making the patient comfortable, ensuring that all injuries have been diagnosed and obtaining an orthopaedic consultation. The nurses and emergency doctors will examine the arm and remove clothing so that the whole arm can be inspected. This may mean that clothes are cut off to prevent further pain or damage to the arm. The examination will pay attention to the site of tenderness, to any deformity of the arm and to the nerve and blood supply of the forearm and hand. X-rays will be taken to show the entire humerus from shoulder to elbow. Normally two views will be taken, an anteroposterior (AP) view from front to back, and a lateral view from the side.
The orthopaedic evaluation of this injury usually takes place after the emergency doctor and team have made the diagnosis. The orthopaedic surgeon will assess the patient's overall medical status and repeat the examination of the arm, paying attention to the nerve and blood supply and any wounds. To form a treatment plan the surgeon will need to review the X-rays and discuss the injury with the patient. This discussion will include the patient's work, life style and expectations as well as the options for treatment and the expected outcome. If there are unusual features such as other major medical problems or a pathological fracture other consultants may be called. It is not usually necessary to take further X-rays of the humerus or to do special tests such as CT scans or MRI.
Our Treatment
What treatments should I consider?
Nonsurgical Treatment
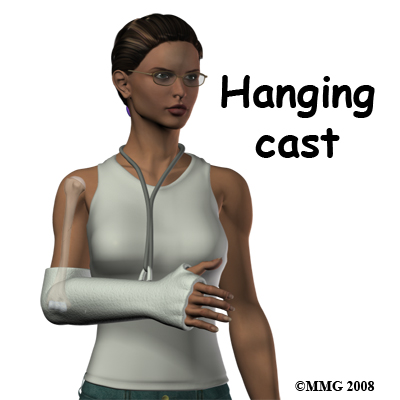 This fracture can often be treated in a cast. The most common type of cast used is the . This cast is applied with the elbow bent at a right angle. The cast goes from above the elbow to the knuckles and prevents movement of the elbow, forearm and wrist, leaving the fingers and thumb free to wiggle.
This fracture can often be treated in a cast. The most common type of cast used is the . This cast is applied with the elbow bent at a right angle. The cast goes from above the elbow to the knuckles and prevents movement of the elbow, forearm and wrist, leaving the fingers and thumb free to wiggle.
The cast is suspended from the neck to a ring attached to the forearm part of the cast. This point of suspension is chosen so that the upper arm hangs straight when the patient is sitting or standing. The cast does not immobilize the fracture but uses the traction from the weight of the hanging cast to position the arm so that the fracture is straight.
During the first few weeks of treatment you can usually feel some movement at the fracture site, particularly when you lie down and the bone tends to bend.
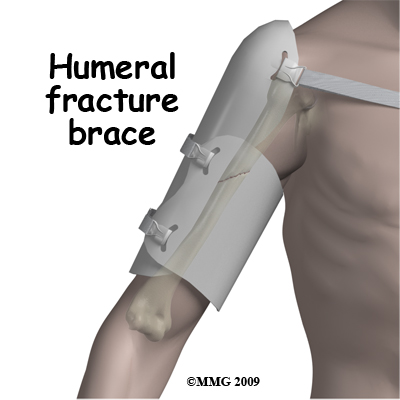
As healing progresses and the tissue at the fracture site gets stronger this sensation of movement goes away. Once the fracture has reached this stage of healing, the cast can be removed. Many surgeons use a removable brace on the upper arm at this stage and continue protection in a sling.
 X-rays are taken frequently during the early part of treatment to make sure that the fracture position is acceptable. By six weeks the healing bone tissue (callus) bridging across the fracture site is mature enough to be seen on x-ray and has about 50% of its eventual strength. This bridging callus is not as strong as normal bone but is a good sign that the bone is healing. By three months post injury the healing bone tissue is about 80% as strong as it needs to be. In terms of function this means that the arm needs protection in a cast or for six weeks or more. After this time frame there should be some limitation of function until three months post injury. This timetable depends on the healing status of the fracture - it may take longer. Return to heavier work or sports activity is less predictable and will depend on the surgeon's assessment of the strength of the healing bone. There is known to be some improvement in the strength of healing bone for as long as 18 months post injury.
X-rays are taken frequently during the early part of treatment to make sure that the fracture position is acceptable. By six weeks the healing bone tissue (callus) bridging across the fracture site is mature enough to be seen on x-ray and has about 50% of its eventual strength. This bridging callus is not as strong as normal bone but is a good sign that the bone is healing. By three months post injury the healing bone tissue is about 80% as strong as it needs to be. In terms of function this means that the arm needs protection in a cast or for six weeks or more. After this time frame there should be some limitation of function until three months post injury. This timetable depends on the healing status of the fracture - it may take longer. Return to heavier work or sports activity is less predictable and will depend on the surgeon's assessment of the strength of the healing bone. There is known to be some improvement in the strength of healing bone for as long as 18 months post injury.
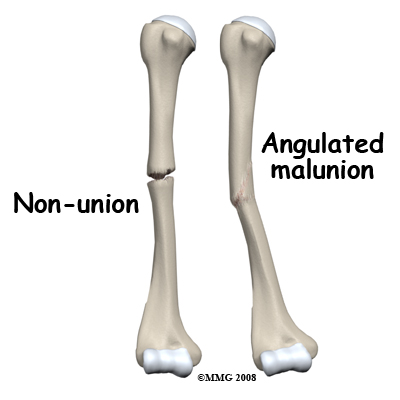
This non-operative method of treating a fracture of the humeral shaft does not usually make the bone completely straight. Due to the excellent range of motion at the shoulder, a degree of angulation at the fracture site does not affect the function of the arm and can be accepted. A small amount of angulation is also cosmetically acceptable because the muscles of the arm hide it.
Surgery
Some situations and some fracture patterns require surgery. Any open fracture needs an operation to wash out all dirty material and remove any dead tissue. It is controversial whether open fractures should be fixed. Some surgeons fix the fracture because they believe that infection is less likely and less damaging if the fracture is held still. Other surgeons do the debridement surgery to clean up the wound but treat the patient in a cast after that, because they believe that minimal interference with the blood supply of an open fracture is better. External fixation with a frame and pins may be used in some open fractures after the debridement surgery.
Another strong indication for surgery is the presence of multiple injuries. If the patient has been in an accident with fractures to the legs or the other arm it may be better to fix the fractured humerus so that the arm can be moved as one. It is very awkward to nurse a patient with a cast on the arm and a broken leg. Using crutches may be difficult until the fractured arm is strong enough. This stage is reached more quickly with surgical fixation.
The third major reason of undertaking surgery to fix a fractured humerus is when the result from non-operative treatment would be un-acceptable in the judgment of the surgeon or after discussion with the patient. Fracture patterns that result in unacceptable malunion or have a very high risk of nonunion would come into this category. The patient may prefer to have surgery in order to speed up recovery.
There are three types of surgery used to fix fractures of the humerus:
- Internal fixation with a plate and screws
- Internal fixation with an intramedullary rod
- External fixation
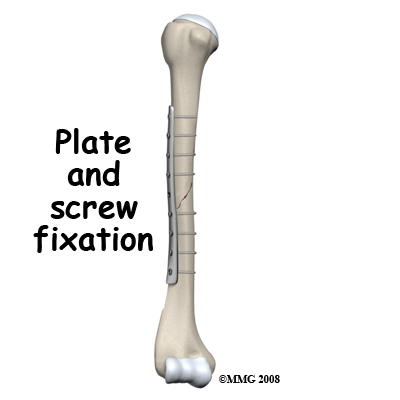 Internal fixation with a plate and screws
Internal fixation with a plate and screws
The operation with requires opening up the fracture, exposing the bone and putting the fragments together, then holding them in place with screws from a metal plate going into the bone. This system affords rigid secure fixation and can also compress the bone fragments together. This aids healing. Exposure of the fracture site makes it possible to reduce the fragments exactly but it does disturb the blood supply of the fracture site. Bone graft can be placed in the fracture site to help healing if considered necessary.
Removal of the implant (plate and screws) may be considered after the fracture has healed and consolidated especially if the site is tender or aching. This operation requires a repeat of the exposure of the site but recovery is much quicker as the bone does not need major healing.
Internal fixation with an intramedullary rod
With fixation (IM rod) of the humerus the fracture is reduced indirectly by manipulation without opening it up.
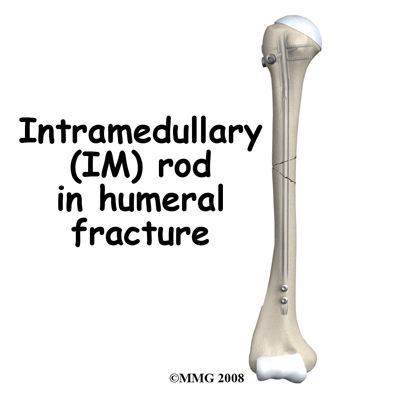
A small exposure is made at the shoulder and a metal rod is inserted into the bone at the shoulder, passed down inside the bone and across the fracture into the lower fragment. This lines up the bone fragments correctly. The bone is held securely by screws passed through the bone and into the rod at both ends.
The main advantage of this method of fixation is that the fracture site is not disturbed so the blood supply of the bone fragments may survive better. It is also very strong mechanically. Technically it is a difficult operation requiring special instruments and an X-ray system to view the fracture during the surgery. The top end of the rod may be irritating and make shoulder movement painful. It is almost always necessary to remove the rod once the fracture has healed. Removal of the rod is a relatively minor operation that does require an anesthetic but is usually done as a day surgery procedure.
External fixation
With , strong metal pins are inserted into the bone fragments above and below the fracture.
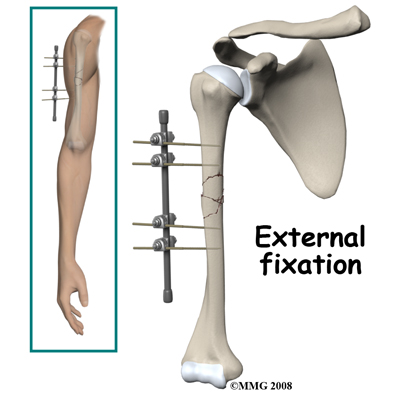 The pins are firmly attached to a frame that spans across the fracture.
The pins are firmly attached to a frame that spans across the fracture.
This holds the fragments immobile while the bone heals. The arm itself can move while in the frame so hand and elbow function does not deteriorate.
Because the alignment of the fracture can be adjusted after the frame has been applied this technique is often used for the more complicated fractures and ones in which there is bone loss.
The disadvantage is a higher incidence of infection where the pins go through the skin.
If this technique is used the pins and the frame are removed as soon as the bone has healed sufficiently.
This procedure does not usually require a general anesthetic. The fracture may need to be protected in a brace for a period after removal of the frame.
Rehabilitation
If your fracture has been casted, rehabilitation with a physiotherapist at Westmount Physiotherapy generally begins once the cast is removed around six weeks post injury. While you are in the cast simple finger movements, neck range of motion exercises as well as pendular exercises to assist with pain and maintain your shoulder range of motion will be your only exercises.
If you have had surgery to fixate your humeral fracture then rehabilitation at Westmount Physiotherapy will begin as soon as your surgeon recommends it. Surgical fixation aims to make the fracture site stable therefore in most cases gentle non-weight bearing exercises to maintain range of motion are safe to do early on and will often be recommended even immediately after surgery. In other cases, rehabilitation will not be recommended until after the bones have shown some evidence of healing on X-ray (usually around six weeks.) Each surgeon will set his own specific restrictions based on the type of fracture, surgical procedure used, personal experience, and whether the fracture is healing as expected.
Even if extensive physiotherapy for your humerus does not begin immediately, at Westmount Physiotherapy we highly recommend maintaining the rest of your body’s fitness with regular exercise. If your humerus has been surgically repaired, maintaining general cardiovascular fitness can be done with lower extremity fitness activities such as walking or using a stationary bike or stepper machine. If your fracture has been casted, activities such as these may need to wait until the bone shows some healing on X-ray as the cast is used more for traction rather than total immobilization. After surgical fixation, weights or weight machines for your lower extremity and opposite arm are also acceptable to use as long as the restrictions regarding your healing humerus are strictly abided by. Generally, lifting any weight with your injured limb will not be allowed and will be difficult as your humerus heals so you may require a friend to assist you with your workout setup if you are keen to continue while your bone heals. Your physiotherapist can discuss the most appropriate way for you to maintain your fitness while abiding by your surgeon’s restrictions and can provide a general fitness program specific to your needs.
When the initial cast is removed or immediately after surgery, you may experience some pain when you start to move your shoulder, wrist, elbow and forearm. If you were in a cast this pain is from not using the joints regularly. If you have had surgery, the pain is likely from the surgical process itself. Your pain may also be from concurrent soft tissue injury that occurred when you fractured your humerus. Your physiotherapist will focus initially on relieving your pain. We may use modalities such as heat, ice, ultrasound, or electrical current to assist with decreasing any pain or swelling you have around the fracture site or anywhere along the arm, into the shoulder or into the hand. Due to some of the muscles of the neck and upper back connecting to the shoulder, you may also have some pain in these regions that we will treat in order to make movement of your entire upper body easier. We may massage the neck, upper back, shoulder, elbow, forearm, or wrist to improve circulation and assist with the pain.
The next part of our treatment will focus on regaining the range of motion, strength, and dexterity in your wrist, hand, elbow, and shoulder. If you have been casted, your arm will look and feel quite weak and atrophied after the cast is removed. Your physiotherapist will prescribe a series of stretching and strengthening exercises that you will practice in the clinic and also learn to do as part of your home exercise program. These exercises may include the use of rehabilitation equipment such as light weights or Theraband that provide added resistance for your upper limb. The shoulder joint is the upper limb’s link to the rest of the body so it needs to be strong and well controlled for the limb and hand to work well. We may also use an upper body bike to encourage coordinated movement of the entire upper limb.
If necessary, your physiotherapist will mobilize your joints. This hands-on technique encourages the stiff joints of your shoulder, elbow, and wrist to move gradually into their normal range of motion. Fortunately, gaining range of motion and strength after a humeral fracture occurs quickly. You will notice improvements in the functioning of your limb even after just a few treatments with your physiotherapist. As your range of motion and strength improve, we will advance your exercises to ensure your rehabilitation is progressing as quickly as your healing fracture allows. Graduated heavier exercises and endurance work will be added in concordance with the known healing time of bone in order to ensure the stresses can be withstood.
As a result of any injury, the receptors in your joints and ligaments that assist with proprioception (the ability to know where your body is without looking at it) decline in function. A period of immobility will add to this decline. Although your humerus is not traditionally thought of as weight-bearing bone, even an activity such as assisting yourself with your arms to get out of a chair or pulling a glass from a cupboard requires weight to be put through or lifted by your humerus and for your body to be proprioceptively aware of your limb. If you are an athlete, then proprioception of your upper extremity is paramount in returning you to sport after a humerus fracture. Your physiotherapist will liaise with your surgeon regarding the optimal time to start exercises that target proprioception by putting weight through the healing humerus bone via the hand. These exercises might include activities such rolling a ball on a surface with your hand, holding a weight up overhead while moving your shoulder, or push- ups on an unstable surface. Advanced exercises will include activities such as ball throwing or catching. For athletes we will encourage exercises that mimic the quick motions of the sports or activities that you enjoy participating in.
Generally, the strength and stiffness one experiences after a humerus fracture responds extremely well to the physiotherapy we provide at Westmount Physiotherapy. With our initial one-on-one physiotherapy treatment along with the ongoing exercises of your home program, the strength, range of motion, endurance and proprioception gradually improve towards near full recovery/function over a period of 3-6 months even though the actual final stages of bone healing won’t occur for another 6-12 months after that. Over time, most patients are able to return to all activities they were doing before the injury. If, however, during rehabilitation your pain continues longer than it should or physiotherapy is not progressing as your physiotherapist would expect, we will ask you to follow-up with your surgeon to confirm that the fracture site is tolerating the rehabilitation well and ensure that there are no hardware issues that may be impeding your recovery.
Westmount Physiotherapy provides services for physiotherapy in Hamilton West Mountain & Ancaster.
Complications
What are the potential complications of this fracture?
Complications after any fracture can include fat embolism syndrome, deep venous thrombosis (DVT), pulmonary embolism and compartment syndrome. Although all of these problems can occur with fractures of the humerus they are not especially common. Complications such as malunion, nonunion, infection, and nerve injury occur more frequently in a humeral fracture so will be discussed here.
Malunion
Unless a fracture has been operated on and fixed, it is rare for the alignment of the fracture to be exactly right. Most often this is acceptable but the angulation or rotation at the fracture site can be great enough to cause problems. This would result in inability to lift the arm fully out to the side or fully forward. Because the arm can rotate a lot these restrictions of motion may not be apparent and so may not need to be corrected. However, if they are significant the malunion can be corrected by surgery. This would normally involve an operation to cut the bone and fix it in the corrected position. This amounts to a new fracture with the same long period of healing so correcting a malunion is not undertaken lightly. If the malunion is treated by surgery one would expect healing and recovery of full range of motion and function.
 Nonunion
Nonunion
Delayed union is said to occur when the fracture has not formed a bridging callus by three months. This is relatively common but there is still a good chance that the fracture will go on to heal. In rare cases, the bone completely fails to heal. This is called . This complication occurs most often after cast treatment as the fracture is not immobilized, but it can also occur after surgery. Other risk factors for nonunion include smoking, multiple fragments, poor blood supply, and infection.
A diagnosis of nonunion is a judgment call on the part of the surgeon; it means that in his/her opinion the fracture will not heal unless some further intervention takes place. Nonunion occurs due to part of the scar tissue that is laid down between the bone fragments failing to turn into bone. The fracture area remains tender and painful, especially when stressed and sometimes movement between the fragments can still be felt. The X-ray shows a persistent gap between the fragments although sometimes it needs a CT scan to demonstrate this.
Nonunion is normally treated by surgery. Scar tissue between the bone fragments is removed and the fracture is rigidly fixated with a plate or IM rod. Bone graft or other substances that stimulate bone healing are frequently used in this situation. The outcome after treatment of nonunion is normally quite good with the bone healing and function being restored. In a very small proportion of cases the nonunion persists and this causes a very difficult problem of management. The two treatment choices include accepting the situation or continuing to investigate a surgical technique that will solve the problem.
Infection
If the fracture is open it is contaminated at the time of the injury and an infection may result. This is likely to interfere with healing of the fracture and may also cause a long-term infection of the bone (chronic osteomyelitis). There is also a small but significant risk of surgical site infection after surgery on a fractured humerus. The wound becomes red, tender and swollen and may discharge pus. The patient often runs a temperature and cultures of the pus or the blood may show evidence of bacteria.
High doses of antibiotics are needed for a long period of time. The surgical treatment is to re-operate on the fracture and clean out any dead or infected tissue including dead bone.
Infection is more likely to take hold when the pressure builds up so opening up the site and creating easy drainage for the pus is an important part of the surgery. Antibiotic beads are often inserted into the wound to create a high local concentration of the drug. If the fracture fixation is stable, the implants may be left in place. Surgeons believe that a stable infected fracture is more likely to heal than an unstable one. In some situations the fixation is removed and external fixation is used instead. Once the infection is under control or eliminated it may be necessary to re-operate to fix the fracture and place bone graft. A combination of infection and nonunion is a severe problem.
Once the fracture is healed the fixation is taken out as the presence of non-living material, such as metal, in the region helps the bacteria to avoid the body's defense system. Infection following a fracture is a serious problem that may require a number of further surgeries. In most cases the outcome is favorable with the bone healed; the infection eliminated, and function of the arm restored. Persistent infection in the bone after healing or infected nonunion can cause long-term problems.
Nerve Injury
Injury to the radial nerve is quite a common complication of a fracture of the shaft of the humerus. It occurs at the time of the fracture when the broken bone ends are tearing through the tissue of the arm. During surgery on the humerus this nerve is also vulnerable to injury.
There is a spectrum of damage from injury to the radial nerve. Stretching or bruising of the nerve may result in temporary problems. If the nerve is not completely severed, this is called axonotomesis. The overall structure of the nerve is intact. The nerve fibers will re-grow and connect up with their target muscles. This takes a long time and it is important to splint the wrist and hand to prevent contraction of the muscle and joints while they are paralyzed. Nerves grow back at a rate of about 1 mm per day so damage to the radial nerve in the upper arm will take several months to recover.
If the nerve is severed, this is called neurotomesis. Where the nerve is cut completely it needs to be repaired so that regenerating nerves have a chance to grow back in the correct direction. Unfortunately, not all of the nerves will grow back to the correct muscles so there will be persistent weakness.
Summary
Fracture of the shaft of the humerus is a serious injury that normally occurs as the result of a significant accident. The bone has a good reputation for healing often without surgery. The bone does not have to heal completely straight to function well and restoration of normal range of motion, strength, and endurance is the usual outcome.
Portions of this document copyright MMG, LLC.









